 A Queer Love Story, a new release from UBC Press, chronicles 15 years of correspondence between gay novelist Jane Rule and The Body Politic editor Rick Bébout. Below is an excerpt from the book, a back-and-forth between Jane and Rick as the pair work on an essay for The Body Politic as the HIV/AIDS crisis was bubbling in Toronto.
A Queer Love Story, a new release from UBC Press, chronicles 15 years of correspondence between gay novelist Jane Rule and The Body Politic editor Rick Bébout. Below is an excerpt from the book, a back-and-forth between Jane and Rick as the pair work on an essay for The Body Politic as the HIV/AIDS crisis was bubbling in Toronto.
These letters provide an eye witness account of the HIV/AIDS crisis in Toronto. Beginning with a New York Times article in July, 1981 titled, “RARE CANCER SEEN IN 41 HOMOSEXUALS,” the disease was soon called GRID (gay related immune deficiency) before becoming known as HIV and AIDS. Rick mentions a “strange flu” circulating in The Body Politic (TBP) office in October 1982. When he was diagnosed in 1988 his doctor said he had probably contracted the virus at that time. Rick’s letters become a personal journal as the disease begins to affect his friends and as TBP responds to the confusion, loss and contradictory advice threatening the community. Fear caused some to see the disease as God’s punishment for deviant sexuality.
In April 1983 Jane sent Rick a draft of an essay titled “An Act of God: AIDS and the Fear of Death,” eventually published in the July/August 1983 issue of TBP:
If AIDS is going to be called an Act of God, I want the phrase interpreted as it is in some insurance policies. I collected 100 percent instead of the usual $50 deductible when my car was damaged by a fire in the engine. For an insurance agent, Acts of God relieve the victim of any responsibility and therefore require total compensation. For god is one of those wanton boys Shakespeare told us about who kill us for their sport. His other names are accident, disease, natural disaster, death.
We live in a country which aspires to universal health care, which declares disaster areas for victims of earthquake and flood, which maintains rescue crews for people stranded in storms at sea, trapped in an aircraft, lost on a mountain. For anybody.
Yet, when something terrible happens, particularly something for which we are helpless, the greatest temptation is to judge the victim. Victims, too, can seek defence against the irrational by looking for something or someone to blame, even themselves; for whatever cold comfort that is, it can seem preferable to facing the fact of random, morally purposeless disaster. . . .
Illness is given moral stigma only when it is related to an activity or a group of people disapproved of.
My niece has five stress fractures in one leg from playing basketball. I wouldn’t play. I wouldn’t climb a mountain either or try to cross an ocean in a small boat or do a lot of other death-defying things so much admired as human achievements, simply for their own sake.
For some men the baths may be what mountains are for others, worth the risk for the view at the top, both the experience and the freedom it symbolizes as good a thing to die for, or of, as any. Many more people die of pleasure, even of the sort reserved for procreation, than is ever reported in the newspapers. Why should it be less admirable than falling in battle, where people are actually trying to kill each other?
It is not the length but the quality of life that matters to me, more easily said now that I am over 50. But it has always been important to me to write one sentence at a time, to live every day as if it were my last and judge it in those terms, often badly, not because it lacked grand gesture or grand passion but because it failed in the daily virtues of self-discipline, kindness, and laughter.
It is love, very ordinary human love, and not fear, which is the good teacher and the wisest judge.
April 1, 1983
Dear Rick:
I have been thinking about your fondness for battle imagery, a way of keeping courage and a sense of importance, and I’m sure that’s why “dying in battle” got into the enclosed essay “An Act of God” about AIDS. I do think it bizarre that we are taught to honor those who die in battle, condemn those who die of pleasure. In the States we early memorize the last words of Nathan Hale, “I regret I have but one life to give to my country.” He didn’t give his life. He gave his death. Giving birth is giving life. There is something basically peculiar about the idea of “dying for other people.” Is there in it a male attempt to equal or transcend the power of giving birth? If only women can do it in this life, only a man can do it for the next? If dying isn’t a punishment, it certainly isn’t a virtue either. I really do want a morality focused on life rather than death.
I must now get back to fiction.
Affectionately,
Jane
3 October 1983
Dear Jane,
The material on war in your essay is very good, and, curiously, reflects a feeling I had just last night when I went to the Albany. One of the bartenders is named Carlos, a man whose intense Latin beauty could be taken to dictate that his role in clone culture would be to stand sullenly against a wall attracting lust and giving nothing in return. In fact, he’s incredibly cheery and physical, rubbing up against people and grinning as he collects empties, dancing with people he knows, taking advantage of the fact that the crowd is small enough that he can relax and actually get to know more people.
There’s a big video screen at the bar, and last night they were showing the first segment of the CBC’s new series on war—tanks rumbling, marching troops, corpses—and all this accompanied by the dance floor’s disco and Carlos—rich, lush, happy Carlos in an ambulatory dance looking for ashtrays to empty. That anybody could ever see him as a “troop,” as one of that mass of expendable bodies to be thrown into these burning fields of mud and machines, that that amazing, warm, alive body could be sent off to become so much carrion—it was all too much to believe. Yet, of course, it’s not too much to believe: that’s how millions and millions of Carloses ended up. It doesn’t all quite make me a pacifist; I think there are situations in which one might have no moral choice but to fight. The horror, I think, is in the massive casualness of it all—all those hundreds of thousands of individual lives turned into faceless soldier-machines, inconvenient refugee problems and innocent civilian targets. All that gets lost except when the CBC shows scenes of war over their happy bodies on the disco floor. It was very curious.
Sincerely,
Rick
]]>
Pierre Trudeau. Bill C-150, passed by his government on May 15, 1969, ushered in a new era of human rights in Canada.
Tomorrow, let’s take a moment to reflect on the 42nd anniversary of the passing of Bill C-150, the omnibus bill that decriminalized abortion, contraception and homosexuality. The rights that Canadians have because of this historic bill are crucial to remember as those same rights come under attack elsewhere: on Wednesday, Indiana became the first state in the U.S. to cut public funding to Planned Parenthood. The same day in Uganda, gay people came close to facing the death penalty.
On May 14, 1969, The Criminal Law Amendment Act formed the legal foundations for the Canadian gay rights movement, and for Henry Morgentaler to perform abortions against — and eventually according to — the law. But it didn’t reduce discrimination, or grant women and members of the LGBTQ community full rights under the charter. Forty-two years later, how much has changed?
Abortion and contraception then:
In the 1950s, a family of five was considered small, explained former nurse Lucie Pepin in her speech commemorating the 30th anniversary of Bill C-150. Many women in rural communities gave birth to their children at home. When complications occurred during birth, the mother was rushed to hospital. If it was too late for a cesarian, her doctor had a decision to make:
“Which to save — the baby or the mother? The Church was clear: save the baby. The Church was clear on many points — women sinned if they refused sexual relations with their husbands or any other form of contraception. The State was also clear. Contraception was illegal and so was abortion.”
Women had no choice in the matter, and neither did their doctors. But Bill C-150 at least changed the latter. The legislation decreed abortion was permissible if a committee of three doctors felt the pregnancy endangered the mental, emotional or physical well-being of the mother. Regard was not given just yet to women’s charter rights to life, liberty and security of the person.
Enter Henry Morgentaler. In 1969, armed with decisive arguments in favour of a woman’s right to an abortion within the first three months of pregnancy, the doctor began performing the procedure illegally in his Montreal clinic. An exchange in 1970 between the adamant doctor and a furious caller on CBC Radio highlighted the fundamental disagreement between the doctor and his critics about when life begins.
Now:
The debate hasn’t progressed. It has degenerated into little more than a shouting match between so-called “pro-life” and “pro-choice” advocates who still can’t agree on when life begins, or whose rights win out: those of the mother or those of the unborn fetus. And recently the Canadian debate has shifted for the worse.
In Indiana, the governor was quite happy to openly chop away at Planned Parenthood’s $2 million in public funding. Meanwhile, in Canada, subtler shifts are taking place. During the election, Tory MP Brad Trost bragged that the Conservative government had successfully cut funding to Planned Parenthood. Stephen Harper quickly denied the comments, saying he would not re-open the abortion debate as long as he is Prime Minister. However, the International Planned Parenthood Federation has been waiting for 18 months to hear whether their funding from the Canadian government will be renewed. During the election, women’s rights groups foreshadowed the Conservatives’ indecision on the matter warning Canadians that Harper would be under pressure from his caucus to re-open the debate. With a Conservative majority now in government, that pressure is sure to grow.
Homosexuality then:
149 Members of Parliament agreed with Trudeau and 55 did not after he famously said “there is no place for the state in the bedrooms of the nation.” According to his omnibus bill, acts of homosexual sex committed in private between consenting adults would no longer be prosecuted. But gay sex between people younger than 21 was still illegal.
A Gallup Poll at the time that asked Canadians whether they thought homosexual sex should be legal or illegal found 42 percent in favour of decriminalization and 41 percent against. Homosexuality was openly discussed as an “illness” that ought to be cured. Progressive Conservative Justice Critic Eldon Woolliams voted in favour of Trudeau’s bill so that gays could have the equal opportunity to receive treatment. On February 2, 1969, he said casually on CBC television:
“I don’t think (homosexuality) should ever be put in the criminal code. I think it should be taken out. It should be done in a medical way so that these people could be sent to centres if we feel as citizens who oppose the feeling of this illness and this homosexuality so they could be rehabilitated.”
Woolliams appeared to sincerely (and incorrectly) believe that gay sex was a mere tendency based on environmental factors, and that the “pressure” of these factors could be “relieved.”
Before Bill C-150 was passed, “incurable” homosexual George Klippert was convicted of “gross indecency.” He was sentenced to preventative detention. In 1967, the Supreme Court upheld the decision.
Now:
Today the Ugandaan Parliament debated a bill that aimed to punish “aggravated homosexuality” by increasing jail sentences from 14 years to life. Until yesterday, the bill also proposed the death penalty for gays. The main motivation behind the legislation was preventing the spread of HIV and AIDS.
We would like to think that Canada is 40 years ahead of Uganda, but we still impose discriminatory policies to prevent the spread of what used to be known as “the gay cancer” — HIV/AIDS.
The policy of the Canadian Blood Services is to ban any man who has had sex with another man since 1977 from giving blood for the rest of his life. The organization asserts that it is arms-length enough from the government to uphold the ban without fear of violating Charter rights. The CBS also discriminates based on action rather than sexuality — a gay man who hasn’t had sex is welcome to give blood. A third argument holds the least strength: though HIV/AIDS testing has advanced over the years, the possibility of a false negative still exists.
However, the policy is inherently discriminatory because it assumes any man who has sex with another man carries a high possibility of illness despite other factors such as relationship status, use of condoms, and differing risk factors based on oral versus anal sex. The CBS, which is regulated by Health Canada, maintains its policy based on outdated science. To their credit, the organization has offered a grant of $500,000 to any researcher(s) who can find a safe way to allow “MSM” men to safely give blood. No researchers have applied for the grant.
The lifetime ban is outdated, as is the recommended deferral period of 10 years, which the U.K. recently implemented. Australia, Sweden and Japan currently have deferral periods of one year. Researchers for the Canadian Medical Association Journal have recommended a one-year deferral policy for MSM donors in stable, monogamous relationships.
We’ve progressed, but we’re not perfect. And there’s a real risk of losing what we have. On May 14, let’s be grateful to the activists that pushed the LGBTQ and women’s rights movements forward.
]]> The March-April 2011 issue of This is now in subscribers’ mailboxes and on newsstands. As usual, you’ll be able to read all the articles here on the website as we post them over the next few weeks. But also as usual, we encourage you to subscribe to the magazine, which is the best way to support this kind of award-winning journalism. You can easily buy a subscription online for one or two years, or we’re happy to take your call at 1-877-999-THIS (8447). It’s toll-free within Canada, and if you call during business hours, it’s likely that a real live human being will answer—we’re old-school like that.
The March-April 2011 issue of This is now in subscribers’ mailboxes and on newsstands. As usual, you’ll be able to read all the articles here on the website as we post them over the next few weeks. But also as usual, we encourage you to subscribe to the magazine, which is the best way to support this kind of award-winning journalism. You can easily buy a subscription online for one or two years, or we’re happy to take your call at 1-877-999-THIS (8447). It’s toll-free within Canada, and if you call during business hours, it’s likely that a real live human being will answer—we’re old-school like that.
Finally, we suggest subscribing to our RSS feed to ensure you never miss a new article going online, and following us on Twitter or becoming a fan on Facebook for updates, new articles and tasty links.
The cover story this issue is Elizabeth Wright‘s look at Canada’s broken drug approval process. The way that pharmaceuticals in this country get approved for medical use is needlessly secretive, rushed, and inefficient, many experts say, and its dysfunction puts everyone’s health at risk. And with Big Pharma in the driver’s seat—from the doctor’s office to the federal research labs, it’s increasingly clear that a more accountable, transparent, and independent drug approval process is necessary.
Also in this issue: Brad Badelt reports on the mystery of B.C.’s 2010 salmon run, which saw record-breaking numbers of fish returning to west-coast rivers. The fish-farming industry said it proved that Pacific salmon stocks are perfectly healthy and there’s no need to worry. But was last year’s boom a sign of resurgence—or a last gasp? Plus we bring you a special eight-page photo essay by Ian Willms from the dark heart of the tar sands. In Fort Chipewyan, 300 kilometres downstream from the world’s most environmentally destructive project, residents are living—and dying—amidst a skyrocketing cancer rate and deteriorating ecosystem.
And there’s plenty more: Paul McLaughlin interviews Silicone Diaries playwright-performer Nina Arsenault; Jason Brown explains how Canada is losing the global race for geothermal energy; Ellen Russell asks why we can’t have more muscular banking reforms; Lisa Xing sends a postcard from Jeju Island, South Korea, where the last of the pacific “mermaids” live; Dylan C. Robertson explains how the Canada-European Comprehensive Economic and Trade Agreement will change our world; Kapil Khatter shows why that “organic farmed fish” you buy may be anything but; Daniel Wilson untangles the right wing’s curious fixation on aboriginal tax exemptions; and Emily Landau sneaks a peek at the next genre-bending project from KENK publisher Pop Sandbox.
PLUS: Christina Palassio on poetry in schools; Navneet Alang on Wikileaks; Jackie Wong on painter Michael Lewis; Flavie Halais on the West Coast’s greenest city; Victoria Salvas on criminalizing HIV-AIDS; Denise Deby on the fight to save Ottawa’s South March Highlands; and reviews of new books by Renee Rodin, Lorna Goodison, David Collier, and David Lester.
This issue also includes debut fiction by Christine Miscione and new poetry by Jim Smith.
]]>
AIDS memorial at 519 Church Street Community Centre, Toronto. Photo courtesy of Kenn Chaplin at Flickr.
Although Pride Toronto decided to reschedule its week-long festivities in light of the G20 circus coming to town, the committee for the AIDS Candlelight Vigil, an event associated with Pride Week, decided it would take advantage of the politically charged atmosphere.
We took the opportunity to speak with Kay Roesslein, co-chair of the AIDS Candlelight Vigil planning committee, about the significance of the event, the decision to keep the original date, and what to expect at this year’s event, which is tonight.
Q&A
Natalie Samson: I was hoping you could tell us about the history and background of the event.
Kay Roesslein: This is the 26th vigil and it truly began for honouring, remembering and celebrating. When it began in the 80s there were so many losses, especially in the gay circles, significant numbers were lost. We saw then over the years [the vigil] become impactful in other communities, including in those wherein substance abuse is a challenge, mental health communities, populations from various countries—that would be the slow progression over the years where losses started to impact [these and] other communities. It really was an opportunity to remember significant losses and to make a statement, to talk about awareness and to raise the flag that HIV is impactful and it can effect us all.
Natalie Samson: So it’s very much a political statement.
Kay Roesslein: Absolutely.
Natalie Samson: Has there historically been any kind of political presence at these vigils?
Kay Roesslein: Not as a rule. June Callwood was here one year and was a host…I know Kyle Rae has attended over the years, George Smitherman has. It’s really a community event. We have strived over the years to keep it a community event. We get sponsorship, yes, but it tends to be sponsorship from [not for profit and related organizations like] Casey House, LOFT Community Services, it’s from ACT [AIDS Committee of Toronto], from the Elementary Teachers Federation. But it’s not from big pharmaceuticals—and that’s intentional. The intent is to keep it a community event.
In fact, the planning committee, all the organizers, are representative from different community agencies or are individuals within the community. That way we stay true, we don’t end up with the politics that we see elsewhere, like Pride, for example.
Natalie Samson: Have you seen questionable sponsorship or politics at other vigils?
Kay Roesslein: I can’t cite any personal examples, no. I am aware though that it came up often in conversation when we looked at our programming, especially with the International AIDS vigil we had during the International AIDS Conference at Yonge and Dundas Square. We invited our local politicians to participate and they did. But again, it’s who do you invite and why, and what’s the message behind it—are we still reflecting our community.
I think one interesting area of growth is the increase in diversity. It speaks to how HIV has grown and impacted so many different communities now. Culturally, it’s all over. So what we’ve done this year, we had to make a decision. We had to decide, because Pride Toronto changed its date, it moved Pride week. Well, if we continued to do the vigil on the Thursday of Pride week, we’d be on Canada Day. We really thought hard about this. Part of us still remains true to the grassroots cause—I mean really it’s still about honouring, celebrating, remembering and awareness. This year, we had wanted to honour those who had died or were affected by HIV/AIDS in those countries where it’s endemic. Of course with the G20 suddenly in town, we had an opportunity to marry our themes. So we are including universal access and human rights as our theme this year. So this year, given that direction around HIV in countries where it’s endemic, the G20 just made sense.
It also influenced our choice around our priority. Our priority is awareness. Our priority is human rights and universal access [to medical treatment]. And given that really we’re talking about HIV, which goes beyond a Pride event, it was appropriate to hold it this Thursday. So we did introduce the G20 [to this event] in this sense. We’re really raising the flag around awareness, saying HIV touches us all; it’s global. We need to look at ourseves in Canada, because there isn’t universal access in Canada. You can ask many aboriginal communities if they feel they have universal access.
Natalie Samson: What’s been the response to keeping the original date?
Kay Roesslein: I think there was consensus by the committee and by the community there’s been absolute understanding. In terms of it being on Canada Day, people understood not competing with that. And as people unraveled the theme of the vigil, especially with our increased diversity on our committee and in our community, it really made sense. If anything has changed over the years, it’s the diversity of our community and the diversity of the board.
Natalie Samson: Is the event run by any particular organization?
Kay Roesslein: We are a Pride event, although that was a little trickier this year because we are not fitting in their calendar since we’re happening just prior to it. So we’re an associated event. We’re associated with the 519 [Church Street Community Centre]. We hold it at the 519 at the AIDS Memorial. We read out the names each year of those who have passed each year and have been put up on the wall.
Natalie Samson: What is the AIDS Memorial at the 519?
Kay Roesslein: It’s a series of upright standing concrete slabs arranged in an arch. There’s a garden around it and it creates a semi-circle. In front of that semi-circle is a flat cemented area and all of this is raised. On each slab that goes around in a semi-circle are metal plaques engraved with names going back to ’84, I believe.
Natalie Samson: How is it decided which names go on the memorial?
Kay Roesslein: We don’t decide. Any name put forward to the AIDS Memorial Committee [through the 519] usually goes up.
Natalie Samson: And it can be an AIDS-related death from any year?
Kay Roesslein: That’s correct. So tonight, for example, we’re reading out names from 1994, 2003, 2007, 2008, and from 2009 and 2010. There are 23 names added this year. They ask for a fee, but where you can’t there is consideration.
Natalie Samson: What can someone expect tonight?
Kay Roesslein: We have Glad Voices that we start with and we end with Singing Out, a huge community choir, and we’ll have about 50 to 60 people on stage at the end. In between we’ll have individual performers on stage…pieces that are really quite touching. But we end with Singing Out on a very hopeful note.
We invite the audience to go on a journey with us wherein first we acknowledge the facts, the gaps, the things that may upset us and make us angry, our call to action and awareness, then we move towards remembering. That’s when we note all the names. And then we move towards honouring with the candle lighting and we move the flame into the audience. It’s quite beautiful.
The AIDS Candlelight Vigil in Toronto will be held tonight, June 24 at 519 Church Street, Cawthra Square Park, from 9-10pm.
]]>
- Year by which G8 countries pledged “universal access” for HIV/AIDS treatment, prevention, and care: 2010
- Estimated number of people, globally, currently receiving that care: 4,000,000
- Estimated number of people, globally, still waiting on that pledge: 5,000,000 *
- Percentage of Canada’s population that is Aboriginal: 4%
- Percentage of new Canadian HIV/AIDS patients who are Aboriginal: 10% *
- Estimated number of Canadians living with HIV/AIDS as of the end of 2008: 65,000
- Percentage increase in number of Canadians living with HIV/AIDS between 2005 and 2008: 14%
- Factor by which an Aboriginal Canadian was more at risk to contract HIV/AIDS in 2008, compared to the general population: 3.6x
- Estimated percentage of Canadian HIV-positive gay men who remain unaware of their infection: 19%
- Estimated percentage of Canadian HIV-positive heterosexuals who remain unaware of their infection (see comment below): 35% *
- Percentage of Catholics surveyed in Ireland, the U.S., and Mexico, respectively, who agreed that “the church’s position on condoms is wrong and should be changed”: 79%, 63%, 60% *
- Estimated amount spent on marketing costs to promote the (Product) RED campaign in its first year: US$100 million
- Amount that Ad Age reported was raised by the campaign for that year: US$18 million *
- Total amount (Product) RED reports it has raised to date, according to a July 2009 blog post: $130 million *
- Year in which HIV/AIDS infections peaked worldwide: 1996
- Global percentage decline in new HIV/AIDS infections in the last eight years: 17% *
- Estimated funds required to respond to the global HIV/AIDS epidemic in 2010: US$25.1 billion *
- Amount by which 2010 funding is currently estimated to fall short of that amount: US$11.3 billion *

In a case before the Ontario Superior Court this month, an Ottawa man is challenging the ban on blood donation by gay men. Currently, any man who has had sex with another man since 1977 is “indefinitely deferred” from giving blood. Not only is this ban unnecessarily broad, it does a disservice to the very people it is supposed to protect.
The reasoning behind the ban is that gay men in Canada account for 60 percent of HIV-positive people, and for nearly half of new infections. All blood collected by Canadian Blood Services is screened for HIV, but the justification for the indefinite deferral of gay men is that the virus is not immediately detectable after infection—it can be several weeks before it shows up on a blood test. Clearly, these are compelling arguments for caution.
Toronto sexual health clinics deal with the issue of detection by waiting three months after a risky sexual encounter to confirm a negative result. Blood agencies in some countries subject gay men and other high-risk groups to a six- or twelve-month deferral period after last sexual contact to make sure the results of screenings are accurate. So why have CBS and Health Canada refused to rethink the total ban?
Another option would be to amend the ban to focus more narrowly on behaviour.
HIV infection rates are higher among gay men, but you are not inherently more likely to wind up with HIV just as a consequence of being gay. You have to have actually engaged in unprotected sex with an infected partner. So why not accept blood from gay men who have not been sexually active for the last six months? Or who have not had unprotected sex? Or who have not had anal sex?
Perhaps CBS simply does not trust gay men to be honest about their activities, in which case we may as well ask why CBS thinks they can be trusted to honestly self-identify at all.
Kyle Freeman, the Ottawa man who launched the current challenge against CBS, claims that asking donors their sexual orientation on their questionnaire is a violation of their Charter rights. In a way though, this isn’t really a fight about queer rights.
An argument could—and has—been made that the policy unfairly portrays gay men in Canada as the harbingers of disease. Or that it spreads misinformation about HIV by implying that it is transmissible by any sexual contact including oral sex, whether you wear a condom or not. But it seems to me that the more pressing issue is about access to blood. CBS has a responsibility to people in need of blood transfusions to provide blood that is safe. But they also have a responsibility to, well, provide blood. Is eliminating every gay man in the country who’s had sex in the last 30 years from the donor pool, when we have the means to make sure that blood is safe, really in the best interests of patients?
 Cate Simpson is a freelance journalist and the web editor for Shameless magazine. She lives in Toronto.
Cate Simpson is a freelance journalist and the web editor for Shameless magazine. She lives in Toronto.
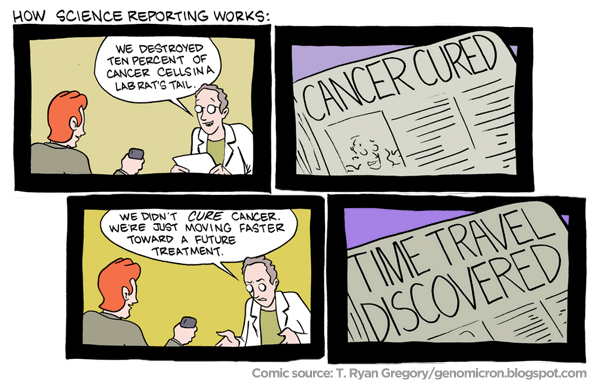
When the news came out yesterday that the largest-ever HIV-AIDS vaccine drug study had concluded with modestly positive results, there was certainly reason to be glad. There was not, of course, any reason to call the damn thing a “miracle vaccine,” as the Dallas Fort-Worth NBC affiliate did. The actual announcement from the U.S. National Institutes of Health, which had conducted the study in Thailand, made no such claims, saying only that the experimental vaccine had a “modest preventative effect”:
In an encouraging development, an investigational vaccine regimen has been shown to be well-tolerated and to have a modest effect in preventing HIV infection in a clinical trial involving more than 16,000 adult participants in Thailand. Following a final analysis of the trial data … the prime-boost investigational vaccine regimen was safe and 31 percent effective in preventing HIV infection.
“These new findings represent an important step forward in HIV vaccine research,” says Anthony S. Fauci, M.D., director of the National Institute of Allergy and Infectious Diseases … “For the first time, an investigational HIV vaccine has demonstrated some ability to prevent HIV infection among vaccinated individuals. Additional research is needed to better understand how this vaccine regimen reduced the risk of HIV infection, but certainly this is an encouraging advance for the HIV vaccine field.
There’s a lot of qualifying language in there: “encouraging development,” “modest effect,” “important step forward,” “some ability,” “additional research is needed,” “encouraging advance,” and of course, that not-exactly-miraculous number, “31 percent effective.” The AIDS Committee of Toronto posted a cautionary tweet late yesterday afternoon, pointing to a somewhat less breathless article that quoted some other AIDS vaccine researchers:
“Wow. Wow,” said AIDS vaccine researcher Ronald Desrosiers, head of the New England Primate Research Center in Southborough, Massachusetts. “Looking at the numbers, it’s underwhelming to me. […] Dennis Burton, an immunologist at the Scripps Research Institute in San Diego, California, had a similar reaction. “It’s very early days,” said Burton. “People should be enormously cautious now.”
So without proclaiming “Cancer Cured!” let’s just say that this is good news, and research will continue, and while we’re waiting for better news, we still have to improve HIV-AIDS education and prevention.
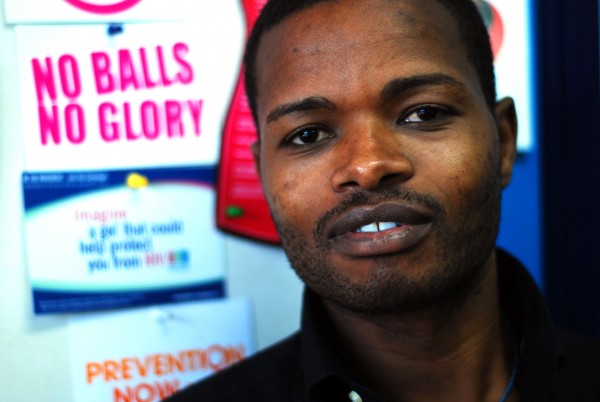
John Mathenke, a Nairobi sex worker, was diagnosed with HIV in early July. He has gone public with his story and started a health education organization to help other young gay sex workers avoid contracting the disease. Photo by Siena Anstis.
John Mathenke was once arrested for being gay but, after failing to pay the customary bribe, was forced to have sex with the policeman. He had an orgy with a priest who publicly excoriates homosexuality, along with five other Masaai boys. And his Arab trader clients curse him during the day, but come back looking for sex at night.
Such is the life of a homosexual prostitute in Nairobi, Kenya. “It’s better to be a thief than a gay in Kenya,” he says. Both are often punished by death, but being the latter means never revealing yourself to the public and remaining perpetually closeted. It means dealing with homophobes at day and pleasuring them at night.
Mathenke, a quiet-spoken young man, is forthright with his story. His gay identity has not been shamed or hidden by years of abuse. His ability to tell his intimate story to a stranger is testament to his bravery. He tells me that he wants to be openly gay – and to help those who want to do the same – in a country where all odds are stacked against him.
His forced silence is not only affecting Kenya’s gay population. According to the BBC, gay men in Africa have 10 times higher HIV rates because of homophobia. These gay men often have “cover wives” who are also eventually affected by HIV. It’s a vicious cycle in a country where the government has proved reluctant to address the mental and physical repercussions of homophobia.
In 2002, Mathenke left his poor community and followed other dream chasers to Nairobi. He paid a barber $30 to be trained as a haircutter. His perfect English eventually landed him a job selling textbooks in a lavish Westlands shopping center. This was the scene of his first same-sex experience. While, subconsciously, he knew it had always been a part of him—he says he used to wear long shirts when he was small and tied a rope around his waist to pretend it was a dress—he had never experienced sex with a man.
A Frenchman would come in, day after day, he says. He would open thick African history books and look at pictures of naked men. He bought many books; some that Mathenke would help him carry to the car. He never thought much of this flirtation, until the man took him out for dinner. Inebriated, they went back to the Frenchman’s home and had sex. The man took him home almost every night after that. In the same store, Mathenke encountered the priest with whom he had a five-person orgy.
At this time, Mathenke was discovering his sexual identity and decided to move to Mombasa, an area rumored to be less hostile to gay relationships. $700 in his pocket, he put himself up in a hotel. Eventually the money dried up and he was left desperate. He went to Mercury, a local bar, and was offered money for sex with an older European.
“When you’ve had sex with someone once, they don’t want you again,” explains Mathenke. Customers became few and far between and he continued to sleep on park benches, washing in the seawater in the morning. He also faced continued stigma: “Arab traders would insult us at day, and come looking for sex at night.” A lot of his clients were—and are—popular religious leaders who would curse homosexuals in public and find pleasure in paid homosexual company in private.
Mathenke eventually returned to Nairobi, where he settled in with a new boyfriend. He continued to see clients from the big hotels: the Hilton, the Serena, the Intercontinental. He had yet to use a condom.
Community outreach by Sex Workers Outreach Program (SWOP) in Nairobi eventually led him to his “second-home.” Provided with free health services and counseling, he tested positive for HIV/AIDS three weeks ago. So did his partner. Instead of bemoaning his future, Mathenke has launched himself into a new project. He is bringing together groups of young gay sex workers and helping them form an advocacy organization, Health Options for Young Men on HIV/AIDS. He is teaching these young men—some only 12 years old—about using condoms and lubricant when having sex with men.
Mathenke’s work is necessary. Many of the bars and hotels on the coast and in Nairobi are, by default, gay bars. The men frequenting these places pay off the police so that they’ll be left alone. But violent raids continue to happen. At the same time, homophobia ensures that these men are never reached by HIV/AIDS awareness. Changing public behavior is key to lowering the HIV rate and protecting all Kenyans, gay or otherwise.
While the government has long been reluctant to address the role of homophobia in increasing HIV/AIDS rates, there have been some positive changes over the years. Gloria Gakaki, a social worker at SWOP, highlights the brave role of Dr. Nicholas Maraguri, Head of the National AIDS and STD Control Programme (NASCOP), who is pushing the government to address HIV among Kenya’s hidden gay populations. Maraguri has also been meeting directly with male sex workers to get a more in-depth idea of what their problems are, and how government can help.
For further information on SWOP or to donate to Mathenke’s new organization, please contact Gloria Gakaki at [email protected].
]]>
Insite provides a vital service for the most marginalized. From Flickr.
A few days ago, a deadline with potentially enormous consequences passed very quietly. Thank goodness. It was June 30th, the day a court order to save Insite – Canada’s only safe injection site for heroine users – was due to expire. Fortunately the government agreed to extend the exemption and allow the facility to continue operating until the B.C. Court of Appeal renders a decision on Insite’s future in the next couple of months.
But for Insite, this is a reprieve and no salvation. The case the plaintiffs have launched in an effort to save the Vancouver facility is a bold one. They argue Insite’s exemption from anti-drug laws isn’t just a good idea; it’s constitutionally protected by the charter right to life, liberty and security of the person. Shut Insite down, they warn, and drug addicts will die. To make their case, they cite the federal government’s own 2008 report. It found that 87 percent of IV drug users on the downtown east side were infected with Hepatitis C and 17 percent with HIV-AIDS. Nearly 60 percent had had a non-fatal overdose – meaning the next time they might not be so lucky. The government side replies, however, that drug laws are reasonable and necessary given the harmful effects of drug addictions on society overall.
Even if Insite wins the appeal this summer, the Conservatives have vowed to take the case to the Supreme Court. This means months or possibly years of legal purgatory for a place that was supposed to be, of all things, secure. And as the legal battle continues, the Conservative PR machine has already started spinning the line that courts are apolitical bodies with no business interfering in the decisions of popularly elected officials on this controversial issue. Let’s pause for a second and ask, what if they’re right? Ultimately, Insite’s future doesn’t depend on a charter right. It depends on funding. And courts forcing the government to fund services is tricky at best, invasive at worst.
Insite has received widespread admiration from national and international civil rights, medical and law enforcement organizations. It is considered the gold standard in addiction treatment. There has never been a single fatal overdose on Insite’s watch. For a group of drug addicts on Vancouver’s east side, that isn’t an accomplishment. It’s a miracle. Moreover, according to the Conservatives’ own polling, 60 percent of Canadians support safe injection sites. The legal case in favour of keeping Insite open may be close, but the political one shouldn’t be.
As Canadians, we rightly celebrate the role courts have in protecting minorities when no one else wants to. But that shouldn’t stop us from fighting long and hard and loud in the political arena . Whatever the courts decide in the next couple months, let’s hope the public outrage is so resounding that the government has no choice to keep Insite open – if not as a question of justice, as a question of politics.
]]>To my eye it’s a bittersweet collection of images: AC-AF, which provided these photos for us to post here, says these photos document the “courage and hope” of the next generation, and you can certainly see some optimism in these images. But the photo that won the contest portion of the program, by a 14-year-old named Warren in Ubungo, Tanzania, strikes me as awfully melancholy — a single student in an otherwise deserted classroom:

Click to see larger version.
There’s an ambivalence to this image—all those empty chairs—that just strikes me as sad. But the point of this isn’t to psychoanalyze every image to death, it’s to get a perspective we don’t often see: life as it’s lived by young people coping with the effects of an epidemic. Click through the jump to see some other images from the series, along with the statements from the kids that accompany their photos.
Click the thumbnails for full-size versions of the photos. Warren’s photo didn’t include a statement, but the other three do. In order, the photos were taken by Zainabu, Yasinta, Thobias, and Warren (last names were scrubbed because all the photographers are under 18)
From the statements that AC-AF took from the kids:
]]>PHOTO 1
Name: Zainabu
Age: 13
What do your pictures show about HIV/AIDS in the future? If AIDS will increase, children will lose their parents and guardians and that will be the beginning of street children and orphans as well. The youth will leave and the country will be empty with only old men who are not capable of working. Animals will miss people to serve them food and water. Plants will wither away because they will lack water, manure and to be well taken care of. Manpower of the nation will disappear. SO IT’S THE DUTY OF EVERY CITIZEN TO PROTECT THE NATION AGAINST AIDS.PHOTO 2
Name: Yasinta
Age: 16
What do your pictures show about HIV/AIDS in the future? Not discriminating the infected, they show that in the future there will be unity. People will not discriminate the people infected from HIV and AIDS. They will love them. They will know they can not transmit a disease by shaking hands, not even by hugging. And when parents give birth they will be educated for those who breastfeed their children to up to three months and when they are given medications for preventing the child from getting transmitted, the parent must tell the truth about her health so that when she is giving birth she should not share the tools when cutting the naval and they should all go for testing and the man should not refuse.PHOTO 3
Name: Thobias
Age: 12
What do your pictures show about HIV/AIDS in the future? The picture shows that HIV and AIDS will increase in a high speed like water from the tap.